What is the Sacro-iliac Joint ?
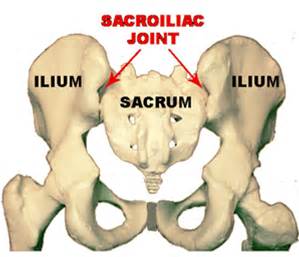
The sacro-iliac joint (SIJ) is a joint formed between the base of the spine (sacrum) and the pelvis (ilium). The SIJ is supported by several large ligaments, which give the joint ability to tolerate large loads. The SIJ is further stabilised by the gluteals and abdominals, which commonly become weak when the SIJ becomes a source of pain.
The SIJ is designed to transfer weight from the ground through the legs and up through the spine. As a result the SIJ only moves a few degrees and is therefore an inherently stable joint.
What is SIJ pain ?
When the SIJ becomes dysfunctional it can cause pain most commonly felt in the buttock or directly over the joint near the dimple in the lower back. The SIJ can occasionally refer pain to the groin or posterior thigh.
Activities that involve loading the SIJ such as single leg standing, rolling in bed, walking and going up stairs can aggravate SIJ dysfunction. Some patients occasionally report clicking or clunking across the SIJ which is due to a lack of muscle control.
Imaging is not often used to diagnose SIJ dysfunction, although bone scans or CT are sometimes used to exclude serious pathology.
Research has shown that physiotherapists can reliably identify the SIJ as a source of pain with a cluster of examination procedures.
What causes SIJ dysfunction ?
Approximately 50% of pregnant women develop pelvic girdle pain and SIJ dysfunction. This is caused by excessive movement across the joint as the ligaments around the SIJ become lax, resulting in SIJ pain.
Trauma to the joint, such as a fall onto the buttocks, can result in strain across the supporting SIJ ligaments and result in SIJ dysfunction.
Inflammatory conditions such as Ankylosing Spondylitis can develop into a condition called Sacro-iliacitis where the SIJ becomes inflamed and irritated. This condition can be diagnosed by your G.P or Rheumatologist.
Reduced muscle support across the SIJ such as weakness in the gluteals and abdominals can predispose the SIJ to excessive strain. Conversely, excessive muscle tone and overactivity can also result in excessive strain across the SIJ.
What treatment is available ?
Treatments that help to stabilise the SIJ such as taping and pelvic belts can give significant relief from SIJ dysfunction. This helps to compress the joint and limits excessive movement. Strengthening programs, in particular those that focus on the gluteals and abdominals have been shown to be effective in reducing pain. Programs emphasising the development of good core strength and movement awareness, such as Physica Active Rehabilitation, are a great way to further progress functional strength.
Manual therapy to mobilise stiff lower back joints or muscle release techniques for tight deep gluteals are also effective in relieving SIJ dysfunction.
Optimising lumbo-pelvic alignment and posture, can also help to reduce strain across the SIJ. Your physiotherapist can re-train this alignment with specific exercises.
Pain relieving injections such as cortisone are used as an adjunct when standard treatments have been in-effective. Sclerosing injections to stiffen the SIJ ligaments are occasionally used as a last line of treatment.
Those conditions related to excessive muscle tension may find relaxation techniques such as meditation and yoga helpful along with specific stretches.
Differential Diagnoses
Structures in the lower back, such as the facet joints or inter-vertebral discs, can refer pain to the SIJ and gluteal region, hence the lower back needs to be thoroughly checked to exclude this as a possible source of pain.
The sciatic nerve is located deep in the buttock and can therefore cause buttock pain. Symptoms such burning, pins and needles and numbness along with pain going down the leg are signs that the Sciatica nerve is involved.
Piriformis syndrome also needs to be excluded as a potential source of pain. This can present similarly to SIJ dysfunction with buttock pain, however, this condition will result in leg pain and possible leg paraesthesia.
Fractures of the sacrum can cause buttock pain, however, these will occur with significant trauma such as a motor vehicle accident.
Inflammatory conditions as mentioned previously, such as Sacro-iliacitis are another source of buttock pain that is systemic in nature and requires medical assessment by a G.P or Rheumatoloogist.
Tips for self managing
- Avoid single leg activities such standing on one leg and stair climbing
- When rolling in bed, use a log roll technique to reduce strain across the SIJ
- Use a pelvic belt throughout the day to compress the joint
- Strengthen the low abdominals and gluteals with specific strength exercises
- Avoid heavy lifting
- Sleep with a pillow between the knees
- Use a lumbar roll when sitting
Return to activity goals
To return to activity, pain levels must be under control with the use of a pelvic belt or specific exercises given by your physiotherapist. Developing full strength in the gluteals and abdominals is essential before returning to dynamic activities such as squatting and lunging. This may take 6-8 weeks of a targeted strengthening regime. Once achieved impact activities such a running and jumping can then be considered depending on pain levels and postural alignment.