Posterolateral Corner Knee Injuries
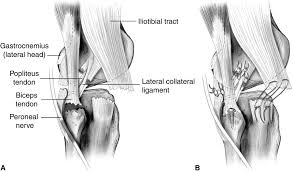
Injuries to the posterolateral corner (PLC) of the knee account for 16% of knee ligament injuries. These type of injuries are complex and frequently overlooked and are commonly associated ACL or PCL injuries. The posterolateral knee has 28 separate structural components. This complex provides both static and dynamic stability to the knee to prevent excessive hyperextension, tibial external rotation and varus angulation. The three most important stabilising structures of the PLC are the popliteus tendon, popliteofibular ligament and fibular collateral ligament (FCL) (Figure 1). Approximately 7-11% of anterior cruciate ligament injuries have an associated PLC injury and if left untreated can cause failure of ACL reconstructive surgery.
History
Patients with PLC injuries may present acutely or chronically and often report a mechanism of injury involving sports trauma, a fall or motor vehicle accident. An associated anterior cruciate ligament (ACL) or posterior cruciate ligament (PCL) tear are not uncommon due to the similar hyperextension mechanism. Acute injuries present with swelling, posterolateral knee pain and occasionally numbness and weakness in the foot as a result of peroneal nerve disruption. Reports of instability within the knee are also common such as ‘giving way’.
Examination
The physical examination needs to be thorough to determine if the PLC is involved in your injury. Your physiotherapist will assess the range of movement in your knee, test your strength and palpate specific structures within the knee. They will also perform a number of special tests to that have been shown to be reliable when assessing the structures of the PLC.
Imaging
Due to the complex anatomy and close proximity of structures imaging may be required. This can assist in identifying specific anatomical structures injured, particularly in acute presentations where the physical examination may be equivocal due to pain and swelling. Magnetic resonance imaging (MRI) is the preferred modality.
Treatment
A conservative approach can be effective and is warranted in less serious injuries. In some cases where the injury is more severe or conservative management has failed to improve symptoms then surgery may need to be considered. Conservative management usually involves a period of immobilization in a brace before commencing a functional rehabilitation program. The first phase of rehabilitation involves regaining full knee movement and strengthening of the quadriceps hamstrings and calf. Neuromuscular re-training (balance re-training) is then added to the program to ensure good hip hip and knee alignment with loading. The last phase of the rehabilitation involves sports specific drills such as running, cutting and agility runs with a gradual return to sport.
Contact one of our clinicians if you have PCL or posterolateral knee injury, all Physica clinicians have undergone further training in the assessment and management of PCL of the knee.