About:
Medial ankle sprains are far less common injuries than lateral ankle sprains and involve injury to the medial ankle ligaments known collectively as the deltoid ligament. This is due to the limited range of movement ankles have into eversion (turning foot out) which is resultant of the lateral malleolus (lateral ankle bone) extending lower than the medial malleolus. Similar to lateral ankle sprains, they are most common amongst running and jumping sports such as AFL, basketball and netball, however they’re also commonly reported as injuries sustained by water skiers.
Symptoms:
- Pain over the medial portion of the ankle – most commonly below the bony prominence known as your medial malleolus
- Pain when walking, running and jumping
- Can present with loss of power in ankle movement secondary to pain
- Feelings of instability when walking/running
- Pain with ankle movements usually involving turning foot outwards
Differential Diagnosis:
Fractures are more commonly involved with medial ankle injuries than they are lateral ankle injuries. Fractures involving the tibia and other bones in the foot such as the navicular, talus and calcaneum can sometimes present concurrently with medial ankle sprains. Fractures may also occur in the fibula as a result of contact from the talus, this is known as a Pott’s fracture. Difficulty weight-bearing can sometimes be an indicator of ankle or foot fractures and in some cases imaging such as x-rays or for some bones CT/MRI scans are appropriate to rule out bony involvement.
Fractures that are most commonly associated with medial ankle sprains are known as avulsion fractures, where a bony fragment where the ligament attaches becomes displaced. These types of fractures, similar to lateral ankle sprains are often managed conservatively in a CAM boot but are also managed surgically if the fragment of medial ligament encroach into the joint space or if pain after being in a boot is persistent.
High ankle sprains are another type of ankle sprain less commonly seen but can present similarly to medial ankle sprains. They often present with pain over the outside of the ankle but also more towards the front and usually don’t involve an inward rolling of the ankle like a lateral ankle sprain. Whilst difficulty weight bearing can also be an indicator, ankle movement inwards is not often painful. This injury involves disruption to either or both the anterior tibiofibular ligament (AITFL) and the syndesmosis (a ligamentous structure responsible for securing your tibia and fibula (shin bones) together.
Causes:
Medial ankle sprains typically occur whilst running or jumping when the foot first contacts the ground again. The ankle is forcefully pushed outwards whilst landing creating a disruption to the medial ligaments. Another common mechanism is when an opponent steps on the outside of the foot/ankle, thus forcing the ankle inwards.

Image - www. vtankletests.weebly.com
The severity of these injuries can differ greatly and is often dependent on the degree of tearing sustained by the medial deltoid ligament complex.
Anatomy and Biomechanics:
The medial ankle ligament complex, also known as the deltoid ligament, involves both deep and superficial components that provide the ankle with medial stability and restrict outwards movement of the foot. The two components are comprised of multiple ligaments listed below:
Superficial deltoid ligament components
- Tibiocalcaneal ligament
- Posterior superficial tibiotalar ligament
- Tibionavicular ligament
Deep deltoid ligament components
- Anterior tibiotalar ligament
- Posterior deep tibiotalar ligament
The deltoid ligament complex is covered over by two tendons, tibialis posterior and flexor digitorum longus, which can also be injured b=via the mechanisms for a medial ankle sprain.
Image - www.earthslab.com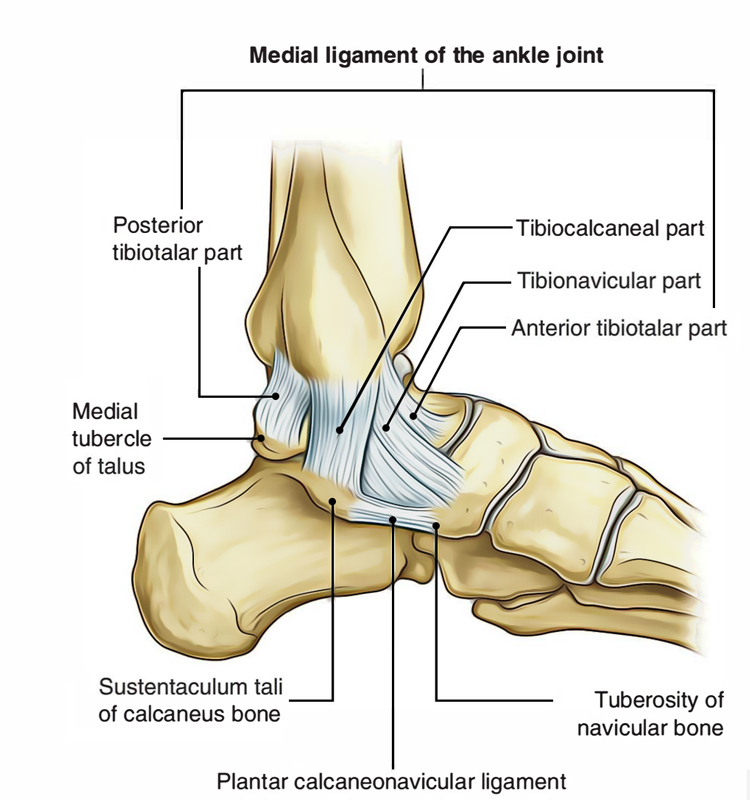{kind=link}

Injury to these ligaments are classified via a grading system similar to other ligaments within the body:
- Grade I: microscopic stretching and disruption of ligament fibres, not commonly seen on macroscopic images such as US or MRI. These injuries are often painful however rarely compromise the medial stability of the ankle.
- Grade II: macroscopic stretching and potentially partial tearing of the ligament which can be seen on imaging. Whilst also painful, these injuries often have associated laxity and minor/moderate compromise of the medial ankle stability.
- Grade III: complete disruption (rupture) of the ligament often leading to moderate/severe compromise to medial ankle stability.
Stability compromise is not only dependent on the degree of injury to the ligament but also varies depending on whether the superficial or deep ligaments are involved.
Treatment:
Medial ankle sprains are most commonly managed conservatively and without surgical intervention. Certainly, for ligament sprains that are classified as grade I or II rarely end up surgically managed.
Initial management usually involves bracing/strapping the ankle to reduce the stretch applied to the medial ligaments and limit inward movement of the ankle/foot. This allows the medial ligaments to stiffen and heal appropriately without repetitively disrupting the acute healing phase. In some cases, this may be done by utilising a CAM boot, which can be more common than the lateral ligaments.
Rehabilitation of medial ankle injuries involves completing strengthening exercises to re-condition the surrounding muscles before returning to activity. A major component of rehabilitation is re-training balance and proprioception.
Proprioception is also known as joint position sense; essentially the process of the nerve endings in your ankle transmitting a signal to your brain to let it know where it is in space, then your brain sending a message to the muscles in your ankle to coordinate movement and maintain you upright. It is re-training balance and proprioception that is important to reduce the future incidence of medial ankle injuries.
In the cases of extreme instability, most commonly occurring via multiple medial ankle sprains, surgical intervention may be required to reconstruct and stabilise these ligaments in order to reduce the risk of osteoarthritis and future ankle injuries. After which, a period of rehabilitation, similar to described above, over a longer period of time is required.