Iliotibial Band Friction Syndrome
Iliotibial band friction syndrome is an injury commonly seen in runners, cyclists and other endurance sports, and typically presents with pain on the outer (lateral) aspect of the knee. This pain may increase with repetitive motion of the knee.
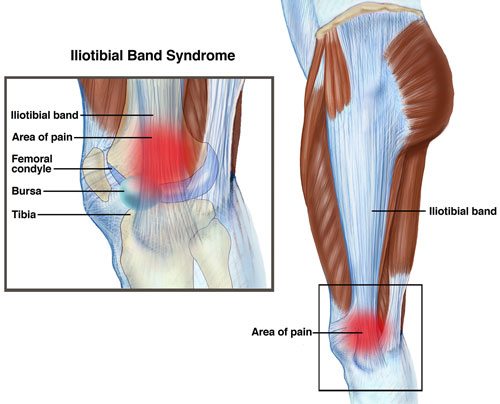
The iliotibial band (ITB) is a band of connective tissue that originates at the hip via two muscles- the tensor fasica lata and gluteus maximus. The ITB runs down the lateral aspect of the thigh and inserts below the knee joint on to the tibia. Structurally the ITB provides support to the outer aspect of the knee and is involved with flexion (bending) and extension (straightening) of the joint.

image taken from www.moveforwardpt.com 23/2/15
Studies have shown ITB friction syndrome can occur in up to 24% of runners and cyclists with it being the most common cause of lateral knee pain in runners. ITB friction syndrome is a non-traumatic overuse injury with multiple factors contributing to the aetiology of the syndrome.
As the name suggests ITB friction syndrome is caused by friction or rubbing of the lower section of the ITB against the lateral femoral epicondyle (knee joint) as the knee is repeatedly flexed and extended. The tight band-like structure can also cause pain by compressing a highly innervated fat pad that lies beneath it.
Physiotherapy management of ITB syndrome has been shown to have a success rate of up to 94%. Early symptomatic relief can be achieved with ice, rest and analgesics. Progressive treatment focuses on soft tissue therapy directed at excessive tightness of the ITB, gluteal muscles, tensor fascia lata and other lower limb muscles. Stretching exercises to improve the flexibility of the hip and leg muscles can also be prescribed.
Specific strengthening of the gluteal and hip musculature can aid in addressing muscle imbalances around the hip and allow proper muscle activation during daily activities and exercise. The patient’s biomechanics should also be addressed, such as excessive subtalar pronation (flat feet) and excessive lateral tilting of the pelvis.
Activity modification plays an important role in the rehabilitation program, with aggravating activities reintroduced in conjunction with appropriate recovery as symptoms improve.
As this injury is multi-factorial, your physiotherapist will conduct a thorough assessment to determine the right management plan for you. If symptoms persist with conservative measures, treatments such as corticosteroid injections or surgery may be discussed.