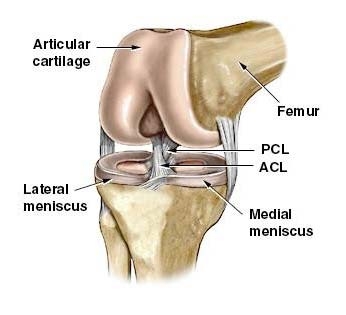
The knee joint is held together by two important ligaments, the anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL). The ACL stops the lower leg moving forward on the thigh and the PCL stops the thigh from moving off the lower leg. They are called the cruciate ligaments because they ‘cross’ each other inside the knee.
The most common mechanism of ACL injury is landing from a jump, pivoting or hyperextension of the knee. The patient usually hears a ‘snap’ or ‘pop’ and the knee often swells immediately with an inability to weight bear.
Tears of the PCL are not as common and often occur from direct contact at the front of the tibia (lower leg) or from hyperextension. Minimal swelling occurs with PCL injuries and the patient can normally weight bear.
Detection of ACL or PCL injuries can be made by your physiotherapist with specific tests. If a structural problem is suspected confirmation can be made with an MRI scan.
Treatment of ACL tears commonly involves surgical repair with either a hamstring graft or patella tendon graft. Rehabilitation is lengthy with the patient returning to competitive sport in twelve months. The first phase consists of controlling swelling and regaining full knee movement. This is followed by developing good muscle strength in the quadriceps, gluteals and calf. Re-training the ‘core’ is often incorporated into the routine. Balance re-training and sports specific drills such as agility running and change in direction are the last phase of the program.
PCL injuries usually respond well to conservative management focussing on quadriceps strengthening and balance re-training.
Surgery may be indicated for ongoing episodes of instability.
All Physica staff are expertly trained in assessing and treating ACL and PCL injuries. The key to an early return to sport is an accurate diagnosis with implementation of sports specific rehabilitation.